
2025
CRI Cancer Immunotherapy Insights + Impact
Executive Summary
The Cancer Research Institute (CRI) Cancer Immunotherapy Insights and Impact report provides a comprehensive analysis of the U.S. Food and Drug Administration (FDA) approvals in cancer immunotherapy from 2011 through the present. This report offers a longitudinal and cross-sectional view of how immune-based therapies have evolved from a nascent treatment modality into a foundational component of standard oncology care.
Since 2011, the field has witnessed a significant expansion in both the volume and diversity of approved immunotherapeutic agents across various treatment indications. Our dataset includes over 150 distinct regulatory approvals, encompassing immune checkpoint inhibitors (ICIs), adoptive cell therapies, cytokine agonists, bispecific T-cell engagers (BiTEs), and novel immune-stimulatory agents.
Here, we map out the rise in total immunotherapy approvals, the cancers most impacted, and the diversification of therapeutic modalities. Notably, the year 2024 alone saw 17 FDA approvals, including first-in-class therapies for melanoma, soft tissue sarcoma, and bladder cancer. In addition, 2024 saw the first approvals for subcutaneous delivery of ICIs to improve access and patient convenience.
The CRI Cancer Immunotherapy Insights and Impact report is an annual resource that provides evidence-based analysis and perspective into where the cancer immunotherapy field is heading, what modalities are gaining traction, and how immunotherapy is evolving toward more personalized, accessible, and durable treatment strategies.
Key Insights
Immunotherapy is a core therapeutic pillar in cancer treatment, with over 150 FDA approvals since 2011 and 17 new approvals in the past year. Today, immunotherapies are available as therapeutic options for over 20 solid tumor indications and five blood cancers.
ICIs continue to dominate as the most common class of immunotherapies, accounting for 81% of currently FDA approved immunotherapies. However, adoptive cell therapies, bispecific antibodies, and next-generation immune agonists are gaining clinical and regulatory momentum.
A real-world dataset indicates the use of FDA-approved cancer immunotherapies has increased more than 20-fold since 2011.
Subcutaneous formulations of ICIs (e.g., nivolumab and atezolizumab) represent a critical shift in administration strategy, improving treatment accessibility and reducing infusion burden for patients and healthcare providers.
The year 2024 marked a pivotal time with the approval of novel modalities, including the first tumor infiltrating lymphocyte (TIL) therapy (lifileucel), the first T-cell receptor (TCR)-engineered therapy for solid tumors (afamitresgene autoleucel), and the first IL-15 agonist (nogapendekin alfa).
Charting the Rise of Immunotherapy
Over the past decade, cancer immunotherapy has evolved from a promising concept into a mainstay of oncology practice, offering new hope amid rising cancer incidence worldwide. Globally, there were an estimated 20 million new cancer cases and 9.7 million cancer deaths in 2022 — a burden projected to swell to 35 million cases by 2050. In the U.S. alone, more than 2 million new cancer diagnoses and over 618,000 cancer deaths are expected in 2025.¹ These statistics underscore the urgent need for more effective and durable treatment strategies.
Unlike traditional treatments such as chemotherapy or radiation, immunotherapy harnesses the body’s own immune system to detect and destroy cancer cells — often with greater precision and the potential for long-term disease control. Since the landmark approval of ipilimumab for the treatment of patients with melanoma in 2011, the field has seen an accelerating pace of innovation, with ICIs, adoptive cell therapies, cytokine agonists, and bispecific antibodies reshaping treatment paradigms across a wide spectrum of malignancies. The number of U.S. FDA approvals for immunotherapies have grown steadily year-over-year, reflecting both the scientific momentum behind immune-based strategies and the increasing number of cancer types for which they are now standard-of-care (Figure 1A).
U.S. FDA-Approved Immunotherapies by Cancer Type (2011-2024)
Figure 1A
Immunotherapies Approved by Cancer Type by Year
BM, biomarker.
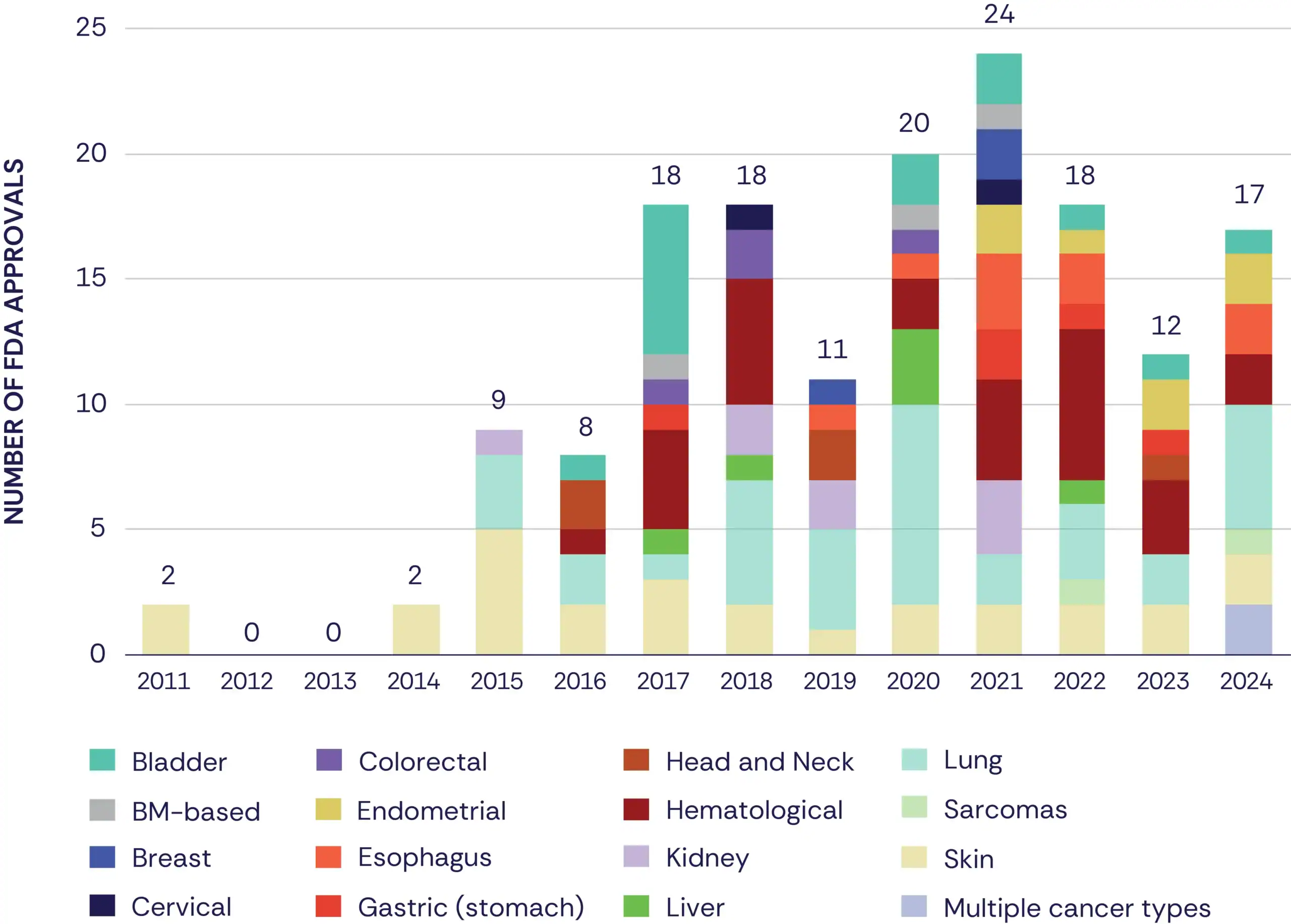
Figure 1B
Immunotherapies Approved by Cancer Type Overall
BM, biomarker.

Lung cancer, hematologic malignancies, and skin cancers — particularly melanoma — account for the highest number of FDA immunotherapy approvals between 2011 and 2024 (Figure 1B). These cancers have historically demonstrated strong immunogenicity, and patients with these cancers were among the earliest to benefit from ICIs and cellular therapies. Bladder and esophagus cancers round out the top five indications, reflecting growing progress for patients with traditionally hard-to-treat diseases and the expansion of immunotherapy for those with earlier disease stages and in combination regimens. These strategies aim to enhance response rates, reduce recurrence, and overcome resistance by pairing immunotherapies with chemotherapy, radiation, or targeted agents.
This rapid expansion of immunotherapy approvals has translated into meaningful changes in clinical practice. Analysis of real-world treatment patterns using de-identified U.S. medical and prescription claims data shows a dramatic rise in the use of FDA-approved cancer immunotherapies, starting in 2015. Usage surged more than 10-fold from 2015 to 2017, coinciding with the broader applicability of ICIs across multiple tumor types, and continued climbing to over 20-fold by 2024. These trends reflect the widespread adoption of cancer immunotherapies and their transformative potential as a cornerstone of modern cancer care.
Modalities in Focus
As the immunotherapy landscape continues to evolve, so too does the diversity of therapeutic modalities entering clinical practice. This growing diversity is illustrated by the classification of all FDA-approved immunotherapies from 2011 to 2024 by their mechanism of action, highlighting the expanding range of immune-based strategies beyond traditional checkpoint blockade (Figure 2A).
ICIs remain the most established and widely applied therapy class in oncology, accounting for 128 approvals (81%, Figure 2B). Within this category, PD-1 and PD-L1 inhibitors constitute the overwhelming majority, making up 91% of all ICI approvals (Figure 2B) and 73% of total immunotherapy approvals during this period. These drugs have become foundational in the treatment of a wide-range of cancers, often serving as the entry point for integrating immunotherapy into standard care. However, the field is steadily expanding beyond ICIs, with growing representation from adoptive cell therapies (15 approvals), including chimeric antigen receptor (CAR) T-cell therapy and TIL based treatments, and bispecific antibodies (10 approvals) that redirect immune cells to tumor targets with precision.
U.S. FDA-Approved Immunotherapies by Modality (2011-2024)
Figure 2A
Immunotherapies Approved by Modality by Year
ICI, immune checkpoint inhibitor.
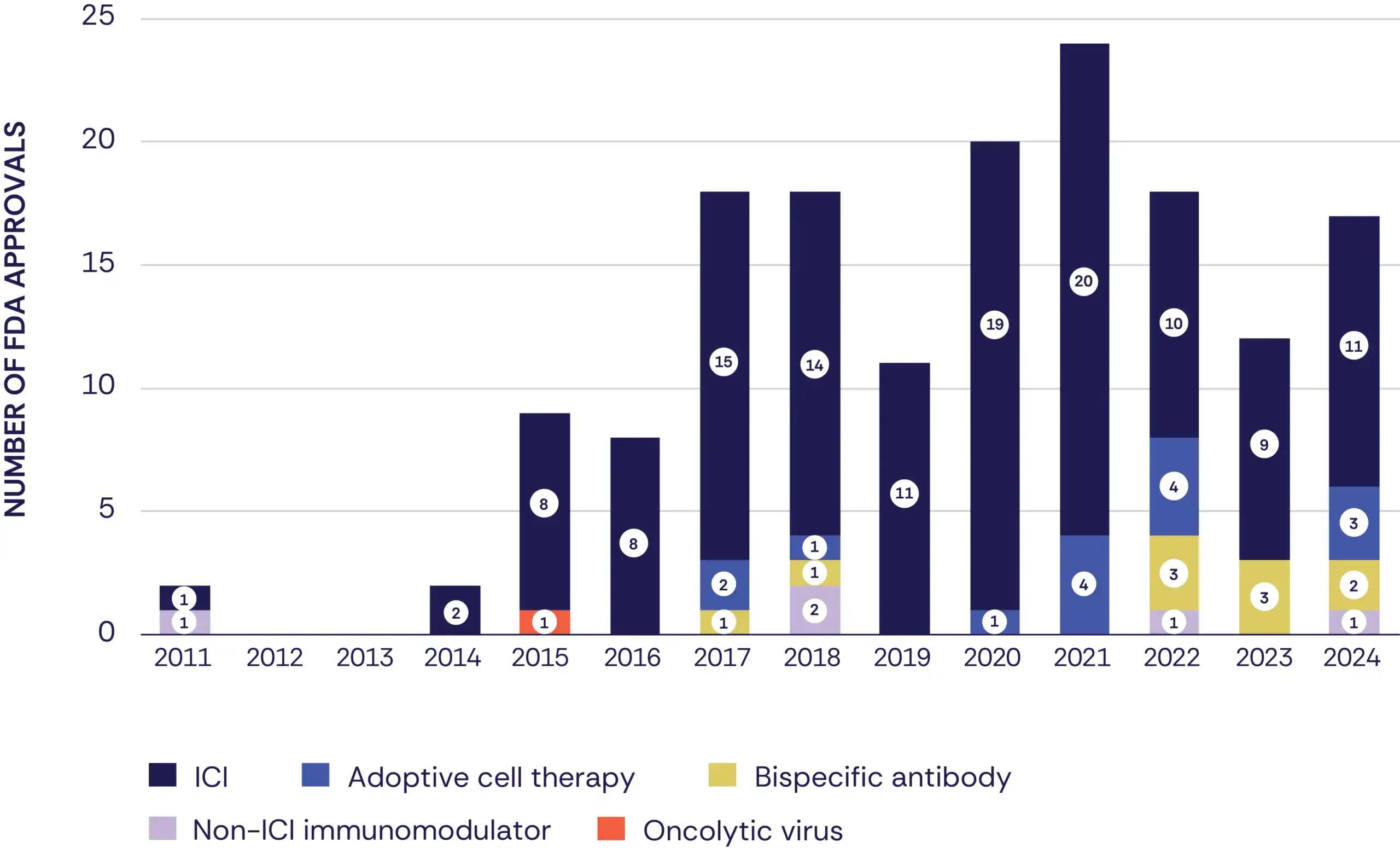
Figure 2B
Immunotherapies Approved by Modality Overall
ICI, immune checkpoint inhibitor.
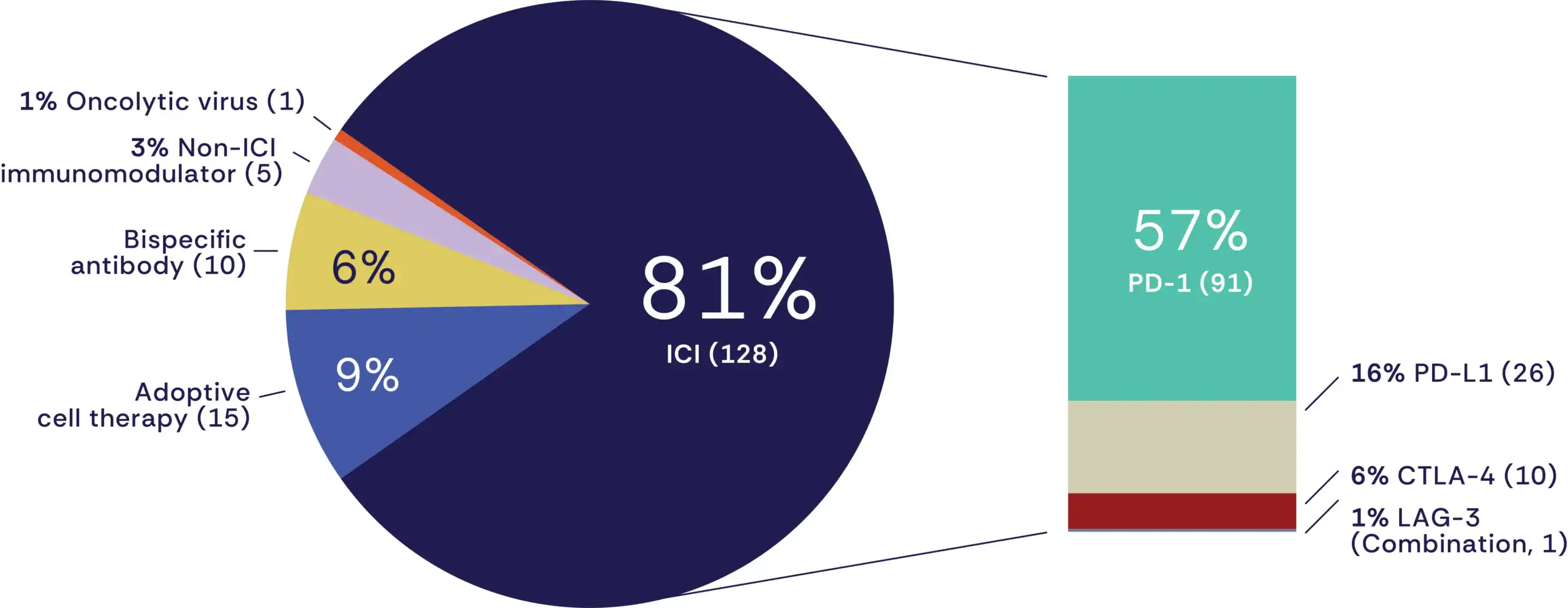
Emerging categories such as non-ICI immunomodulators (five approvals), which include cytokine agonists like interleukin (IL)-2 and IL-15 analogs, and oncolytic viruses (one approval) signal the field’s shift toward novel immune activating strategies. This evolving therapeutic mix underscores a broadening of immunotherapy’s toolkit, with the next-generation of agents poised to complement or extend the reach of traditional checkpoint blockade, especially in resistant or less immunogenic cancers. Table 1 lists all immunotherapy approvals from 2011 to 2024 across cancer types.
2024 FDA Approval Highlights
In 2024, the FDA continued to expand the landscape of cancer immunotherapy, approving several novel agents and indications. These advances included first-in-class therapies for patients with previously untreatable cancers and expanded uses of established ICIs, including in patients with earlier disease stages and in combination regimens.
Together, these approvals reflect a broader evolution in the field — one that is shifting from monotherapy to combination strategies, from late-stage interventions to earlier, more proactive treatment, and from generalized use to biomarker-guided precision medicine. This transition underscores a maturing immunotherapy pipeline that is becoming more personalized, strategic, and integrated across the continuum of cancer care. These advancements offer new hope for patients across a range of malignancies and highlight ongoing progress in harnessing the immune system to combat cancer.
Top 5 Cancer Types with the Most U.S. FDA Immunotherapy Approvals
1
Lung cancers tend to have a high mutation burden, making tumors more visible to the immune system.
2
Hematologic cancers offer clear immune targets like CD19, enabling success with cell therapies.
3
Skin cancers, notably melanoma, are highly immunogenic and led to early checkpoint inhibitor advances.
4
Bladder cancer’s long-known immune sensitivity makes it a natural candidate for newer immunotherapy approaches.
5
Esophageal cancer is often diagnosed in an advanced stage, and ICI therapies expand treatment options.
2024 by the Numbers
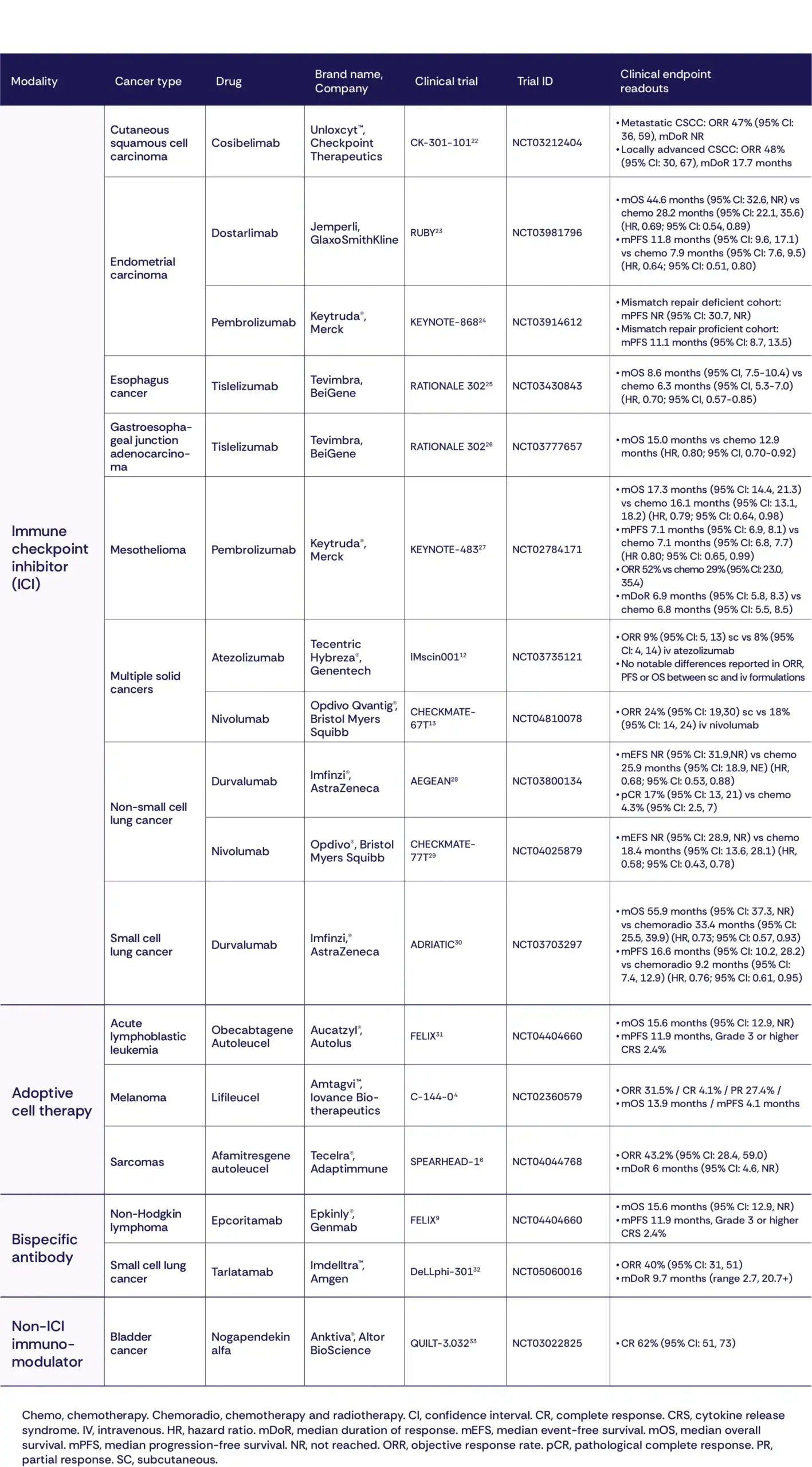
The FDA granted 17 immunotherapy approvals in 2024, continuing the upward trajectory of immune-based oncology treatments (Table 2). The approvals spanned four distinct therapeutic modalities, reinforcing the diversification of the field:
- A total of 11 were ICIs, including both new indications and updated formulations;
- Three were adoptive cell therapies, reflecting growing momentum in solid tumor applications, where historic challenges such as tumor heterogeneity and the immunosuppressive microenvironment have limited efficacy;
- Two approvals were for bispecific antibodies, signaling continued investment in precision immune targeting; and
- One approval represented a non-ICI immunomodulator, a key milestone in advancing next-generation immune stimulants.
This distribution highlights how ICIs remain the backbone of cancer immunotherapy, while newer modalities are beginning to carve out their place, especially for patients with cancers historically resistant to standard immunotherapy approaches. The growing diversity of the immunotherapy pipeline reflects a field that is not just expanding but evolving – embracing a wider range of mechanisms, modalities, and disease contexts.
As the treatment landscape shifts beyond single-agent therapies, it is increasingly clear that monotherapies alone are rarely sufficient. Cancer’s inherent complexity and heterogeneity demand coordinated, multi-pronged strategies that can adapt to the unique biology of each tumor and patient.
This broadening of therapeutic strategies is reflected in several landmark FDA approvals in 2024, which highlight how next-generation immunotherapies are advancing beyond conventional checkpoints. From novel cell therapies and bispecific antibodies to immune agonists and innovative delivery formats, these approvals exemplify the field’s shift toward more personalized, potent, and accessible treatment options.
Historic Firsts
In February 2024, the FDA granted accelerated approval to the first TIL therapy, lifileucel (Amtagvi™), marking a significant step forward for cell therapies targeting solid tumors. While CAR T-cell therapies have revolutionized treatment for certain blood cancers, adoptive cell therapies have historically faced major obstacles in solid tumors, owing to the complexity of the tumor microenvironment, difficulty in targeting tumor-specific antigens, and the physical barriers that limit immune cell infiltration. TIL therapy seeks to overcome these challenges by expanding a patient’s own tumor-infiltrating T cells outside the body and subsequently reinfusing them to amplify the immune response (Figure 3).
Figure 3
Schematics of the Three Novel Immunotherapy Modalities Approved in 2024

The approval of lifileucel is particularly significant in the context of advanced melanoma, a disease that remains highly lethal despite representing only a small fraction of overall skin cancer cases. Invasive melanoma accounts for just 1% of all skin cancers but causes the vast majority of skin cancer deaths, with an estimated 104,960 new cases and 8,430 deaths expected in the U.S. in 2025.¹ Lifileucel’s approval represents the culmination of decades of research and clinical development that was first validated in 1988 through early work led by Dr. Steven Rosenberg at the National Cancer Institute.³
The FDA’s approval decision was supported by results from the phase II C-144-01 clinical trial,⁴ which enrolled patients with advanced melanoma who had progressed despite treatment with PD-1/PD-L1 checkpoint inhibitors or targeted therapies. Among 73 patients treated with lifileucel at the recommended dose, the overall response rate was 32%, including a 4% complete response rate. Notably, 44% of responses lasted at least 12 months, supporting lifileucel’s potential for durable clinical benefit.³ A phase III trial combining lifileucel with the PD-1 inhibitor pembrolizumab (Keytruda®) is ongoing to confirm its long-term efficacy.⁵
In another landmark decision in August 2024, the FDA granted accelerated approval to afamitresgene autoleucel (afami-cel, Tecelra®), the first TCR-engineered therapy targeting a solid tumor antigen (MAGE-A4) for the treatment of unresectable or metastatic synovial sarcoma, a rare and aggressive cancer.⁶ Afami-cel represents a new generation of personalized cell therapies designed to recognize intracellular tumor antigens presented by human leukocyte antigen (HLA) molecules, expanding immunotherapy’s reach beyond surface-expressed targets (Figure 3). This approval marks the first genetically engineered TCR therapy for a solid tumor and builds on years of translational research into adoptive T-cell platforms.
The approval of afami-cel was based on data from the phase II SPEARHEAD-1 clinical trial,⁶ which enrolled patients with advanced synovial sarcoma who had exhausted standard therapies. Among 42 patients treated with afami-cel, the overall response rate was 43%. Of the 19 patients who responded to the treatment, two achieved complete responses, with no evidence of disease recurrence during the three-year study period. This approval underscores the potential for engineered cell therapies to target intracellular antigens in solid tumors — an area that has historically proven difficult to treat. Emerging next-generation candidates building on this platform are already showing early signs of efficacy in other solid tumor types,⁷ laying the groundwork for a new wave of more effective and broadly applicable TCR-based therapies.
Bispecific Antibodies Gain Momentum
Bispecific antibodies have emerged as a novel and increasingly prominent immunotherapy modality, offering targeted immune activation with off-the-shelf convenience. Since the FDA’s first full approval of a bispecific antibody — blinatumomab (Blincyto®) in 2017 for relapsed or refractory B-cell precursor acute lymphoblastic leukemia — the field has seen growing clinical interest and development. In 2024, this momentum continued with the FDA’s accelerated approval of epcoritamab-bysp (Epkinly™) for adults with relapsed or refractory follicular lymphoma (FL) after two or more prior lines of therapy. FL is the second most common subtype of non-Hodgkin lymphoma, with an estimated 15,000 new cases diagnosed annually in the U.S.⁸ This marks the second accelerated approval for epcoritamab, following its 2023 indication for diffuse large B-cell lymphoma. Epcoritamab is a BiTE designed to bind simultaneously to CD20 on malignant B cells and CD3 on T cells, redirecting T cells to eliminate cancerous cells. Administered subcutaneously and available as an off-the-shelf product, it offers a more accessible and manageable alternative to complex cell therapies for B-cell malignancies.
The latest approval was based on data from the phase I/II EPCORE NHL-1 clinical trial,⁹ wherein epcoritamab demonstrated an overall response rate of 82% and a complete response rate of 60% among patients with relapsed or refractory FL. Importantly, subcutaneous delivery helped mitigate severe cytokine release syndrome, an immune-related complication often associated with T-cell engaging therapies that can cause symptoms ranging from fever and fatigue to life-threatening organ dysfunction. By mitigating these risks, subcutaneous administration not only improves the safety profile but also enables treatment to be delivered outside of major academic centers, including in community clinics. As confirmatory trials continue, epcoritamab reflects the growing momentum of bispecific antibodies as a versatile and scalable approach within the immunotherapy toolkit.
First-in-Class for Bladder Cancer
In April 2024, the FDA granted accelerated approval to nogapendekin alfa inbakicept-pmln (Anktiva®), in combination with Bacillus Calmette-Guérin (BCG), for the treatment of adults with non-muscle invasive bladder cancer (NMIBC) that is unresponsive to BCG alone. This indication addresses a meaningful clinical need: in 2025, bladder cancer accounted for approximately 85,000 new cases and 17,000 deaths in the U.S., with NMIBC comprising the majority of new diagnoses.¹ The approval marks an important milestone, not only for introducing the first IL-15-based immune agonist into treatment, but also for building on the legacy of BCG, which became one of the earliest FDA-approved cancer immunotherapies when it was authorized for bladder cancer in 1990.²
Nogapendekin alfa inbakicept-pmln works by activating the IL-15 pathway to stimulate the proliferation and activation of key immune effectors, including CD8+ T cells and natural killer (NK) cells, enhancing the body’s ability to mount a sustained anti-tumor immune response (Figure 3). Unlike ICIs that release immune brakes, nogapendekin alfa inbakicept-pmln acts as an immune amplifier. When combined with BCG, this novel approach aims to reignite immune responses in patients who have exhausted frontline therapy options. The approval was based on data from the phase II/III QUILT-3.032 clinical trial,¹⁰ where 62% of 77 treated patients achieved a complete response. Of those, 58% maintained their response for at least 12 months, and 40% sustained it for at least 2 years, underscoring the potential for durable clinical benefit. With limited alternatives short of bladder removal for these patients,¹¹ nogapendekin alfa inbakicept-pmln introduces a promising new strategy that could redefine care for BCG-unresponsive NMIBC.
Advancing Access Through Subcutaneous Delivery
In parallel with first-in-class innovations, 2024 also marked significant progress in improving the accessibility and patient experience of ICI therapies. The FDA-approved subcutaneous formulations of two widely used PD-L1 and PD-1 inhibitors: atezolizumab (Tecentriq Hybreza™) and nivolumab (Opdivo Qvantig™),¹²,¹³ which have traditionally been administered via intravenous (IV) infusion. These new subcutaneous formulations offer significantly faster delivery — about seven minutes for atezolizumab (vs. 30–60 minutes IV) and under five minutes for nivolumab (vs. 30 minutes IV) — while maintaining comparable drug profile and clinical efficacy.¹⁴,¹⁵
Approved for use across nearly all indications previously granted to their IV counterparts, these subcutaneous versions cover a broad range of cancers. Atezolizumab is now available in subcutaneous form for malignancies including non-small cell lung cancer (NSCLC), small cell lung cancer (SCLC), hepatocellular carcinoma, and melanoma, while nivolumab’s approvals span more than a dozen tumor types, including renal cell carcinoma, melanoma, NSCLC, and multiple gastrointestinal cancers. These developments not only streamline delivery in oncology clinics but also lay the groundwork for future home-based or low-resource setting administration, which is especially critical in expanding access to patients in healthcare deserts. As immune checkpoint blockade continues to be a foundational pillar of cancer treatment, innovations in formulation and delivery are poised to enhance patient convenience, reduce healthcare burden, and support more flexible care models.
Eyes on the Horizon for 2025
Looking towards the cancer immunotherapy landscape for 2025, there are several emerging trends to watch closely in the coming year.
KRAS-Targeted Cancer Vaccines
In the past two years, there have been advancements in the development of mutant-specific KRAS-targeting vaccines for the treatment of patients with pancreatic ductal adenocarcinoma and colorectal cancer. These vaccines aim to train the immune system to recognize frequently occurring KRAS mutations which are common in these diseases. The promise of this vaccine strategy is in its ability to offer a tailored treatment option while maintaining off-the-shelf availability. Initial phase I studies have demonstrated that these therapies are tolerated and are able to generate KRAS-specific T-cell responses,¹⁶ and phase II studies are actively recruiting to examine their efficacy and durability. It is anticipated that several of these studies will be read out in the coming year and could unlock a new paradigm for cancer vaccine development.
Immunotherapy as a Neoadjuvant Strategy
Most immunotherapy studies to date have focused on combining ICIs with standard treatments such as surgery, radiation, or chemotherapy. However, a study published this year suggests that checkpoint blockade alone may be sufficient to non-operatively manage certain solid tumors.¹⁷ This phase II trial evaluated the use of dostarlimab (Jemperli, a PD-1 ICI) as a neoadjuvant therapy for patients with mismatch repair-deficient (dMMR) tumors. Remarkably, the study found that in some cases, dostarlimab alone led to complete clinical responses, eliminating the need for surgery. If these outcomes prove durable, this approach could represent a major shift in cancer care: a non-invasive, immunotherapy-first strategy for managing dMMR solid tumors, reducing the need for surgery and improving quality of life for patients.
A Two-Pronged Approach to NSCLC
Building on highly promising data from early clinical trials in China, the field is eagerly anticipating the full results read-out of several HARMONi studies. These phase III trials are evaluating the efficacy of ivonescimab (a novel PD-1/VEGF bispecific antibody) across multiple NSCLC settings. Ivonescimab’s dual-targeting mechanism addresses both immune evasion and tumor angiogenesis and has already shown striking clinical activity. In the HARMONi-A study, ivonescimab is being tested in combination with chemotherapy versus chemotherapy alone, as a second-line treatment for patients with epithelial growth factor receptor (EGFR)-mutated advanced or metastatic non-squamous NSCLC. Early data have shown that the ivonescimab-plus-chemotherapy regimen reduced the risk of disease progression by 54% and the risk of death by 20% compared to chemotherapy alone.¹⁸
In a separate phase III trial, HARMONi-2, ivonescimab monotherapy was evaluated against pembrolizumab in PD-L1-positive NSCLC. Data presented at the 2024 IASLC World Conference on Lung Cancer showed that ivonescimab lowered the risk of progression by 49% as compared to pembrolizumab.¹⁹ Based on these data, ivonescimab received approvals from China’s National Medical Products Administration for marketing in China. The approvals encompass two indications: 1) as a monotherapy for the first-line treatment of patients with PD-L1-positive NSCLC and 2) in combination with chemotherapy for patients with epidermal growth factor receptor (EGFR)-mutated locally advanced or metastatic non-squamous NSCLC who have progressed on EGFR tyrosine kinase inhibitor therapy.²⁰ With these compelling early signals, anticipation is high to see whether the full HARMONi trial will confirm ivonescimab’s potential to reshape treatment paradigms in this challenging patient population.
China’s Expanding Role
A key trend that has emerged over the past year has been the growing global influence of Chinese innovation in developing novel drug therapies in immuno-oncology and beyond. A Stifel report released at the beginning of 2025 indicated that more than a third of the therapeutic molecules bought by pharmaceutical companies came from China in 2024, an all-time high.¹¹ In addition, promising preclinical and early clinical trial data continues to come from Chinese companies, including the ivonescimab data detailed above. With these trends, it is anticipated that there will be more early discovery breakthroughs to be seen in the coming year.
ICIs, adoptive cell therapies, non-ICI immunomodulators, bispecific antibodies, and oncolytic viruses) and by cancer type. The data were manually curated and verified across multiple official sources for accuracy and completeness.
This report does not include data from international regulatory bodies, which may constrain the global applicability of findings. While FDA approval data were curated from official public sources, the dynamic nature of regulatory activity, such as label expansions, withdrawals, or new formulations, may introduce lags or omissions in the dataset. Additionally, the analysis does not account for off-label use or variations in clinical practice patterns.
Conclusions
The story of cancer immunotherapy is far from complete. What was once a bold concept is now a cornerstone of oncology treatment. In 2025, we expect the next chapters to be defined not just by what immune therapies can do alone, but how they work together, guided by biology, data, and patient-centered innovation.
Methods and Limitations
FDA Approval Data
This analysis was conducted using publicly available data on U.S. FDA approvals of cancer immunotherapies from 2011 through 2024. Primary data sources included FDA approval announcements, prescribing information, regulatory review documents, and publicly reported clinical trial results. Immunotherapies were categorized by therapeutic modality (e.g., ICIs, adoptive cell therapies, non-ICI immunomodulators, bispecific antibodies, and oncolytic viruses) and by cancer type. The data were manually curated and verified across multiple official sources for accuracy and completeness.
This report does not include data from international regulatory bodies, which may constrain the global applicability of findings. While FDA approval data were curated from official public sources, the dynamic nature of regulatory activity, such as label expansions, withdrawals, or new formulations, may introduce lags or omissions in the dataset. Additionally, the analysis does not account for off-label use or variations in clinical practice patterns.
Real-World Data
To assess trends in the clinical adoption of immunotherapy, de-identified patient-level medical and prescription claims data were analyzed using IQVIA’s U.S. database. The analysis assessed the number of unique patients with claims records for defined immunotherapies each year from 2011 through 2024. Additional analyses from 2019 to 2024 quantified the number of treated patients by cancer type and by immunotherapy class.
The analysis is subject to limitations inherent in the U.S. healthcare data; variability in healthcare access, reimbursement, and coding practices across institutions introduces heterogeneity that may result in underrepresentation of total immunotherapy usage. As such, findings are best interpreted as directional indicators of adoption trends rather than precise population-level totals
Acknowledgments
The Cancer Research Institute extends its sincere appreciation to Mark Raupp and Jeffrey Hodge of IQVIA for their valuable collaboration in providing real-world data and expert insights that informed the analysis presented in this report.
TABLE 1: FDA-Approved Immunotherapies by Cancer Type by Year
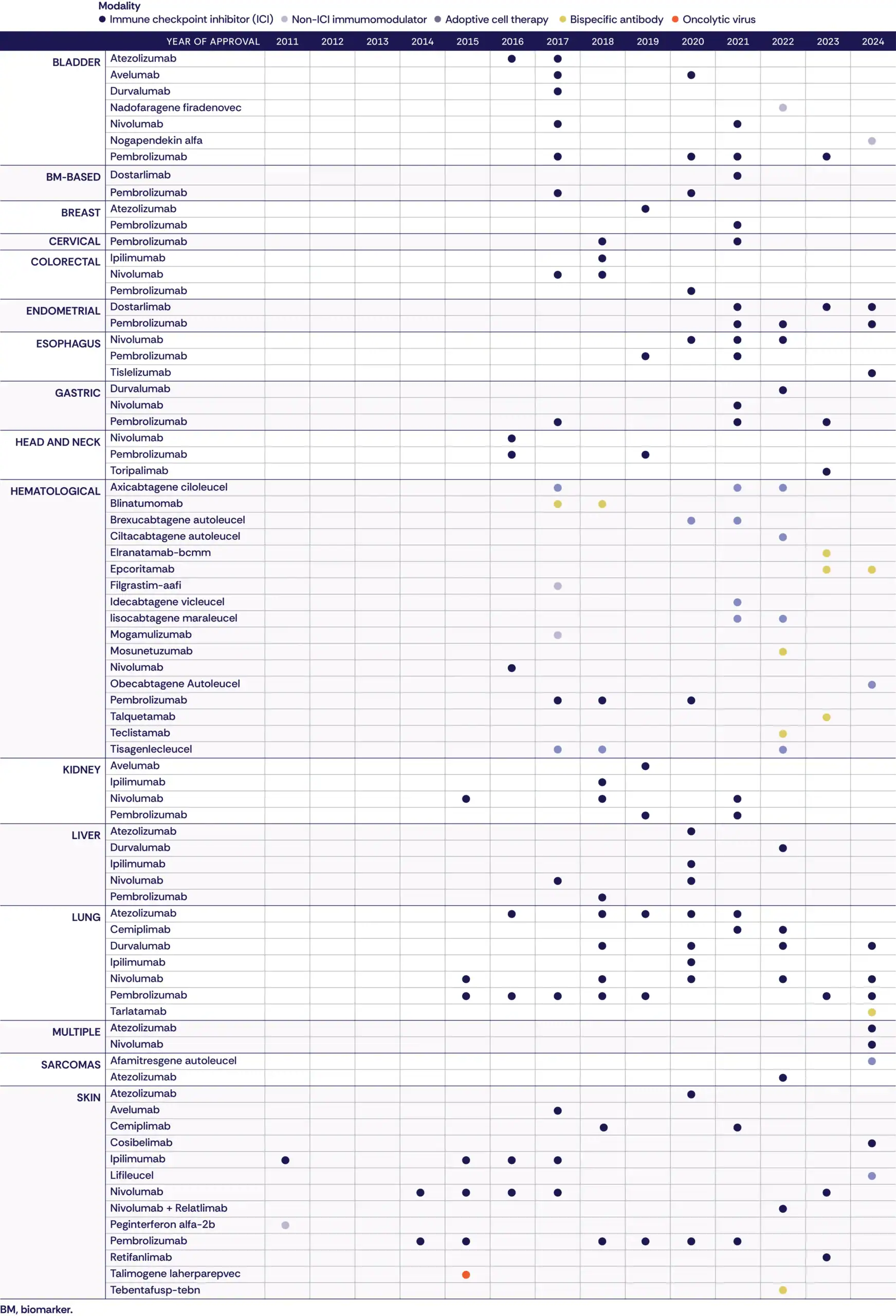
TABLE 2: Clinical Trial Endpoints of Immunotherapies Approved by the FDA in 2024
References
- Surveillance and Health Equity Science. Cancer Facts & Figures 2025. American Cancer Society, Inc.; 2025. Accessed March 10, 2025.
- Lobo N, Brooks NA, Zlotta AR, et al. 100 years of Bacillus Calmette-Guérin immunotherapy: from cattle to COVID-19. Nat Rev Urol. 2021;18(10):611-622.
- Rosenberg SA, Packard BS, Aebersold PM, et al. Use of tumor-infiltrating lymphocytes and interleukin-2 in the immunotherapy of patients with metastatic melanoma. A preliminary report. N Engl J Med. 1988;319(25):1676-1680.
- FDA Approves First Cellular Therapy to Treat Patients with Unresectable or Metastatic Melanoma. U.S. FDA. August 9, 2024. Accessed May 12, 2025.
- Study to Investigate Lifileucel Regimen Plus Pembrolizumab Compared With Pembrolizumab Alone in Participants With Untreated Advanced Melanoma. ClinicalTrials.gov. Accessed May 19, 2025.
- FDA Approves First Gene Therapy to Treat Adults with Metastatic Synovial Sarcoma. U.S. FDA. August 9, 2024. Accessed May 12, 2025.
- Aggen DH, Garcia A, Saro Suarez JM, et al. New phase 1 SURPASS trial cohort: Early-line ADP-A2M4CD8 T-cell receptor T-cell therapy plus pembrolizumab in urothelial carcinoma. J Clin Oncol. 2024;42(4_suppl):TPS708-TPS708.
- Leukemia & Lymphoma Society. Follicular Lymphoma (FL). Accessed May 12, 2025.
- FDA grants accelerated approval to epcoritamab-bysp for relapsed or refractory follicular lymphoma. U.S. FDA. June 26, 2024. Accessed May 12, 2025.
- FDA approves nogapendekin alfa inbakicept-pmln for BCG-unresponsive non-muscle invasive bladder cancer. U.S. FDA. August 9, 2024. Accessed May 12, 2025.
- Matulewicz RS, Steinberg GD. Non-muscle-invasive bladder cancer: Overview and contemporary treatment landscape of neoadjuvant chemoablative therapies. Rev Urol. 2020;22( 2):43-51.
- FDA approves atezolizumab and hyaluronidase-tqjs for subcutaneous injection. U.S. FDA. September 12, 2024. Accessed May 19, 2025.
- FDA approves nivolumab and hyaluronidase-nvhy for subcutaneous injection. U.S. FDA. December 27, 2024. Accessed May 19, 2025
- FDA Approves Injectable Nivolumab, an Alternative to IV Infusion. National Cancer Institute. February 19, 2025. Accessed May 19, 2025.
- New Atezolizumab Formulation for Subcutaneous Injection. American Association for Cancer Research. September 12, 2024. Accessed May 19, 2025
- Damle SR, Pillarisetty VG, Safyan RA, Chiorean EG. A new dawn in cancer immunotherapy: the promise of mutant KRAS-specific vaccines. Transl Gastroenterol Hepatol. 2025;10:20.
- Cercek A, Foote MB, Rousseau B, et al. Nonoperative management of mismatch repair-deficient tumors. N Engl J Med. Published online April 27, 2025. doi:10.1056/NEJMoa2404512
- Ivonescimab in Combination with Chemotherapy Approved in China by NMPA for 2L+ EGFRm NSCLC based on HARMONi-A Clinical Trial: Positive Trend Observed in Overall Survival towards Ivonescimab Plus Chemotherapy. Akeso News. Accessed May 19, 2025.
- Ivonescimab Outperforms Pembrolizumab in Phase 3 Study for First-Line Treatment of PD-L1-Positive Advanced NSCLC In HARMONi-2 Study. International Association for the Study of Lung Cancer. Accessed May 19, 2025.
- Ryan C. Ivonescimab Wins NMPA Approval in China for First-Line, PD-L1+ Advanced NSCLC. OncLive. April 28, 2025. Accessed May 20, 2025
- Biopharmaceutical Outlook for 2025. Stifel, Nicolaus & Company; 2025. Accessed May 12, 2025.
- FDA approves cosibelimab-ipdl for metastatic or locally advanced cutaneous squamous cell carcinoma. U.S. FDA. December 13, 2024. Accessed May 19, 2025.
- FDA expands endometrial cancer indication for dostarlimab-gxly with chemotherapy. U.S. FDA. August 1, 2024. Accessed May 12, 2025.
- FDA approves pembrolizumab with chemotherapy for primary advanced or recurrent endometrial carcinoma. U.S. FDA. June 17, 2024. Accessed May 19, 2025.
- FDA Approves Tislelizumab for Advanced or Metastatic ESCC After Chemotherapy. OncLive. March 14, 2024. Accessed May 19, 2025.
- FDA Approves Tislelizumab Plus Chemo for PD-L1+ Unresectable or Metastatic Gastric/GEJ Cancer. OncLive. December 27, 2024. Accessed May 19, 2025.
- FDA approves pembrolizumab with chemotherapy for unresectable advanced or metastatic malignant pleural mesothelioma. U.S. FDA. September 17, 2024. Accessed May 19, 2025.
- FDA approves neoadjuvant/adjuvant durvalumab for resectable non-small cell lung cancer. U.S. FDA. August 15, 2024. Accessed May 19, 2025.
- FDA approves neoadjuvant/adjuvant nivolumab for resectable non-small cell lung cancer. U.S. FDA. October 3, 2024. Accessed May 12, 2025.
- FDA approves durvalumab for limited-stage small cell lung cancer. U.S. FDA. December 4, 2024. Accessed May 19, 2025
- FDA approves obecabtagene autoleucel for adults with relapsed or refractory B-cell precursor acute lymphoblastic leukemia. U.S. FDA. November 8, 2024. Accessed May 19, 2025.
- FDA grants accelerated approval to tarlatamab-dlle for extensive stage small cell lung cancer. U.S. FDA. May 16, 2024. Accessed May 19, 2025.
- FDA approves nogapendekin alfa inbakicept-pmln for BCG-unresponsive non-muscle invasive bladder cancer. U.S. Food and Drug Administration. April 22, 2024. Accessed May 19, 2025.
Discover Resources for Researchers

Explore the IO Landscape Dashboard
Use our interactive dashboard to review and track the full set of FDA-approved cancer immunotherapies. Explore trends across drug class, target, indication and pathway.
Connect Data to Discovery
Learn how CRI Data Programs help researchers transform complex biological datasets into actionable insights and ultimately immunotherapy treatments.

Advance Your Research with CRI
Review funding opportunities for early-career, mid-career, translational, and clinical immunotherapy researchers.

Keep Up-To-Date with Ongoing Research
Stay informed through our IO Insights Newsletter, connect with us at scientific conferences and hear about the latest grant funding opportunities.