
Earlier this year, the Cancer Research Institute (CRI) announced the second class of its ambitious Lloyd J. Old STAR program, named in honor of the “Father of Modern Tumor Immunology.”
One of these promising STARs (Scientists Taking Risks) is Joshua D. Brody, MD, an associate professor of medicine, hematology, and medical oncology at the Icahn School of Medicine at Mount Sinai in New York City. Recently, we spoke with Dr. Brody, who was also a CRI CLIP Investigator from 2015 to 2017, to learn more about his work and ambitions as a CRI Lloyd J. Old STAR.

Arthur N. Brodsky, PhD:
Vaccines have long been a crucial component in our healthcare arsenal, especially against infectious diseases. They’re also being studied as a way to fight cancer. What types of cancer vaccines are there?
Joshua Brody, MD:
In general, a vaccine is just a combination of some antigens, which are markers that enable the immune system to recognize cells, plus an immunostimulant that tells the immune system that these antigens are bad and stimulates immune responses against them.
Most people when they hear the word vaccine, they imagine a preventive or prophylactic vaccine because all the ones we use for infectious diseases—tetanus, measles, mumps, rubella, etc.—act to prevent disease. Some, like the human papillomavirus (HPV) vaccine, can prevent the development of cervical cancers and head and neck cancers caused by HPV infection.
But vaccines can also be therapeutic and treat a problem that’s already there. In cancer, therapeutic vaccines can teach your immune system to recognize a tumor that’s already developed. But what tumors targets do we go after with vaccines, since everyone’s cancer is essentially different?
There are a number of common antigens that might make good targets for cancer vaccines. WT1, MUC 1, and HER2 are some examples of antigens that can be expressed by both normal cells and cancer cells, although tumors often express them at higher levels. But no one antigen is ideal because tumors can often evade the immune system by getting rid of that antigen. Not many of these antigens by themselves are essential to the survival of the cancer cells.
Another approach is to go after what are called neoantigens. These neoantigens, which can result from mutations or viral infection, are only expressed by tumor cells. We can use our tools to discover the specific neoantigens that an individual’s tumor has, predict which ones might make the best targets for the immune system, and then make a personalized vaccine for them. This is very elegant, but extremely resource-intensive.
Lastly, there is an approach that my team is exploring called in situ vaccination or ISV. Instead of creating the vaccine in the laboratory or in a factory, we create the vaccine right at the tumor site. We vaccinate against the entire tumor and it requires no processing and no personalization. Each patient’s tumor is stimulated in such a way that it creates its own vaccine with the tumor environment. That allows us to induce T cells against neoantigens, but without having to identify them beforehand, although we can identify them afterwards. We’ve shown this works in mice, and now we’re testing the approach in clinical trials for humans with cancer.
With this ISV approach, one of the keys is that we activate immune cells called dendritic cells. This could be done, for example, by using radiation therapy to kill some tumor cells and alert the immune system. Then we can add agents that activate the Flt3 and Toll-like receptor (TLR) pathways, both which are important in stimulating dendritic cells and adaptive immune responses.
Arthur N. Brodsky, PhD:
It sounds like your ISV strategy stimulates the immune system to do what it’s already designed to do naturally. You just jumpstart the process.
Joshua Brody, MD:
Yes, definitely. We co-opt what the immune system is naturally designed to do, which is eliminate threats. The immune system is designed primarily to fight off bacteria and viruses, but we can co-opt that whole armamentarium to fight cancer.
These infectious agents generally pack some of the immune-stimulating molecules that activate dendritic cells, such as those that trigger the TLR pathway, on their own, but cancer doesn’t. That’s why we have to supply them via injection into the tumor.
Arthur N. Brodsky, PhD:
That’s a creative strategy. I understand you’re also looking at how vaccines might work well in combination with another type of immunotherapy called checkpoint inhibition or checkpoint blockade.
Joshua Brody, MD:
First, I’d just like to note that checkpoint blockade is the greatest advance in cancer immunotherapy ever, and yet still it does not help the majority of our patients, so clearly a lot of improvement is needed.
If the immune cells—the T cells—that kill cancer are automobiles, then checkpoint inhibition is akin to cutting the brakes of those automobiles. From the perspective of cancer immunotherapy, that’s great because we want these T cell cars to keep driving and going after cancer. But for the best chance of success, we also need the gas pedal and the steering wheel. And that is what the vaccine provides. It is the steering wheel which tells the T cells which antigens to go after and pushes the gas pedal, so it helps drive those T cells forward.
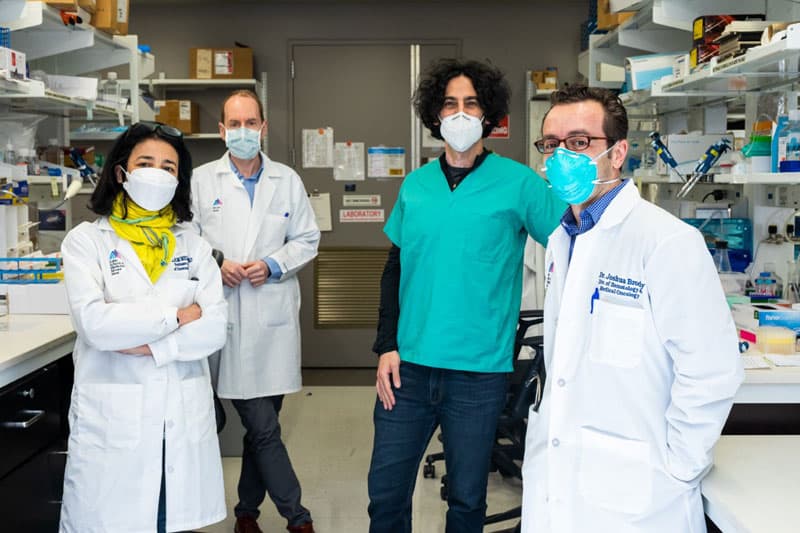
The team at the Precision Immunology Institute at Mount Sinai has been tackling both cancer and COVID-19. Left-to-right: Miriam Merad, MD, PhD; Sacha Gnjatic, PhD; Brian D. Brown, PhD; Joshua D. Brody, MD Photo courtesy of Brian Brown
Arthur N. Brodsky, PhD:
Do you think this strategy could also be effective in human cancers?
Joshua Brody, MD:
Yes, I believe it could. That’s why we’re now testing that combination in a clinical trial that opened recently for patients with lymphoma, breast cancer, and head and neck cancer. We have treated a few patients so far but cannot speak to the results yet.
Arthur N. Brodsky, PhD:
We look forward to hearing them eventually.
I want to hop to another part of your work now. Earlier, you alluded to a phenomenon known as antigen escape. As you mentioned, T cells recognize cancer cells by the antigens they express. But, if a cancer loses certain antigens, this can essentially make them invisible to T cells.
Recently, you found that the Fas pathway can re-sensitize cancer cells to T cell killing, even if they don’t have those antigens targets anymore, as long as other cells nearby do. What do we know about the mechanisms of this process and how it might work?
Joshua Brody, MD:
Antigen escape is probably the greatest common weakness of almost all types of cancer immunotherapy, meaning checkpoint immunotherapy, CAR T cell therapy, and bispecific antibodies, which are probably the three types of immunotherapy with the greatest impact for the foreseeable future.
One of the ways we are trying to address antigen escape is by taking advantage of the Fas pathway, whose receptor is expressed at high levels in many cancers. What we’ve found is that if a T cell kills a cancer cell, it can also kill the cell just next door or even maybe a cell a few cells away by binding to the Fas receptor.
Fas allows for this “bystander” killing even if the bystander cell, the cell next door, has lost the target antigen. But if Fas is lost, then the T cell is totally unable to kill that adjacent cell. So maybe we could increase Fas signaling using some standard medicines and increase bystander killing in that way.
Arthur N. Brodsky, PhD:
Gotcha. So, in addition to optimizing your ISV approach, you’ll also be focusing on developing these Fas-based strategies as part of your CRI Lloyd J. Old STAR work. To that end, what are your some of your next steps?
Joshua Brody, MD:
Well, there’s a couple of low hanging fruits. The obvious approaches I just hinted at, that use some of these Fas-targeting therapies in combination with some of these immunotherapies to prevent the problem of antigen escape.
The truth is, though, we probably won’t see the patient benefit there immediately because these antigen escape problems are problems that really occur later, in the advanced stages of tumor progression. That’s why the therapies stop working over time, so our real goal here is to see if we can prevent antigen escape and hopefully improve the durability of these clinical responses.
Arthur N. Brodsky, PhD:
That makes a lot of sense. How important is this CRI Lloyd J. Old STAR funding in your pursuit of this goal?
Joshua Brody, MD:
It’s no understatement to say that this funding is absolutely critical to pushing these ideas and concepts forward to become therapies for our patients. We have been fortunate to get some funding from the National Institutes of Health (NIH), but that has been extremely difficult because we’re at an all-time low in terms of the proportion of scientists and doctors that get federal funding for biomedical research.
We can’t afford to wait for NIH funding for some of these ideas though, especially the early ideas. That will slow the pace at which we can advance these ideas into the clinic, and will completely prevent some of them from being developed, especially for small to medium-sized labs like mine that cannot continue our work without consistent funds.
Industry funding is another potential source, but it comes with its own agenda where the science is generally intended to discover something about the specific therapy in which the funder is interested. The NIH and industry can both be great funding sources, but the funding from the Cancer Research Institute is absolutely different. It expedites our ability to try to translate these new immunotherapy strategies to the clinic, as we have been able to do before with CRI’s help. Some examples include trials investigating vaccines, both alone and in combination with checkpoint immunotherapy, as well as other immune-based treatments.
So, this CRI funding will not only expedite our ability to translate discoveries into clinical trials, but also enable us to salvage and develop some of these approaches that would be relegated to the dustbin if it weren’t for the funding.
Joshua D. Brody, MD, and his lab at the Icahn School of Medicine at Mount Sinai in 2013.
Arthur N. Brodsky, PhD:
What do you hope that you will be able accomplish over the next five years with this CRI funding?
Joshua Brody, MD:
We hope to show that the combination of ISV with checkpoint inhibition—which was so potent in mice—also works in humans who have lymphoma, breast cancer, and head and neck cancer. Additionally, we hope to develop a better understanding of how ISV works, and which strategies might complement it best, so that we can optimize these therapeutic approaches and bring them to patients with other types of cancer.
Lastly, we want to improve our knowledge of how antigen escape occurs and potential treatments to counter it. Then, in the next couple years, we might be able to bring those into early phase clinical trials for our patients receiving those standard immunotherapies in order to boost their effectiveness.
